Head & Neck
Sinus and Nasal Cancer
Includes illustrated staging details
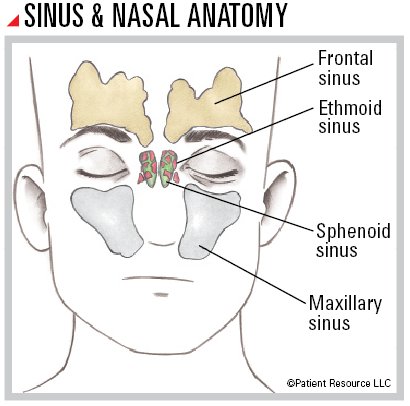
The sinuses and the nasal cavity work together to filter, warm and moisten the air you breathe before it reaches your lungs. Cells in the sinuses make mucus to keep your nose from drying out.
The nose leads into the nasal cavity, which is divided by your septum (dividing wall of the nose) into two passages. Your nasal cavity is a space that extends above the roof of your mouth and into the passageway from your mouth to your throat.
You have four paranasal sinuses: in the hollow spaces in the bones around your nose; behind your cheekbones; above, below and between your eyes; and in the center of your skull. Named for the bones that surround them, they are the frontal, ethmoid, sphenoid and maxillary sinuses.
Cancer typically develops in thin, flat squamous (SKWAY-mus) cells lining the sinuses and nasal cavity. The most common place for this type of cancer to occur is in the maxillary sinuses.
Treatment Options
Your treatment plan will be determined based on the stage of the disease and your age, overall health, symptoms, previous treatments and preferences for quality of life. One or more of the following therapies may be recommended.
Surgery is frequently used to remove any stage of sinus and nasal cancer. It may be the only treatment needed for early-stage cancer. During surgery, the cancer will be removed along with an area of normal tissue around it and some surrounding bone or other nearby tissues. It may also be used if the cancer is found in the nasal cavity. If the tumor is found in the septum, the whole septum may be removed.
Multiple types of surgery are available. Your doctor will consider the location and stage of your cancer to choose the appropriate surgery for you.
Many early sinus and nasal cancers can be removed endoscopically (with a thin, lighted camera and instruments designed to pass through the nose) and do not require incisions on the face. However, many advanced tumors will require external incisions for adequate removal.
Medial maxillectomy may be used to treat a tumor in the sidewall of the nasal cavity and may involve removing the sidewall.
Maxillectomy may be done if the tumor has grown into the maxillary sinus. A maxillectomy may involve removal of bone from the roof of the mouth, part or all of the eye socket, part of the cheekbone, upper teeth and/or the bony part of the upper nose. In very advanced cancers that involve the eye itself, an exenteration, which includes removal of the eye, may be necessary.
Endoscopic ethmoidectomy may be used if the tumor is small and found only in the ethmoid sinuses. This involves the use of an endoscope (a thin, lighted camera) to reach the ethmoid sinuses through the nose. In some cases, it is necessary to make an incision (cut) between the nasal bridge and the eye to reach the ethmoid sinuses. This is called an external ethmoidectomy.
Craniofacial resection may be done if the cancer is found in the ethmoid, frontal and/or sphenoid sinuses. This surgery is more extensive than a maxillectomy because it can include removal of the upper parts of the eye socket and front of the skull base.
A neck dissection (removal of lymph nodes in the neck) is often performed, regardless of whether the cancer is in the sinus or nasal cavity:
- A selective neck dissection involves removal of lymph nodes from a limited area of the neck.
- A modified radical neck dissection involves removal of most of the lymph nodes on one side of the neck between the jawbone and collarbone, in addition to some muscle and nerve tissue.
- A radical neck dissection involves removal of nearly all of the lymph nodes on one side of the neck and even more muscle, nerves and veins.
Reconstructive surgery may be needed after the primary surgery to restore functional ability and/or appearance. Missing tissue, skin or bone may be replaced during this surgery (see Reconstruction & Rehabilitation).
Radiation therapy may be the main treatment if your general health is too poor for surgery. It is generally used for cancers in the sphenoid sinuses because these areas are difficult to reach surgically. It can be used after surgery as adjuvant treatment. It may also be combined with chemotherapy (chemo- radiation). Radiation delivery methods vary by type and stage of cancer.
External-beam radiation therapy (EBRT) is delivered by a machine outside of the body. Types of this treatment include three-dimensional conformal radiation therapy (3D-CRT) and intensity-modulated radiation therapy (IMRT).
Proton therapy uses protons instead of X-rays and may benefit some patients, depending on the location of the tumor.
Drug therapy may be given alone or in combination with other therapies.
Chemotherapy may be given before surgery as neoadjuvant therapy or after surgery as adjuvant therapy. It may be combined with radiation therapy (chemoradiation). It is usually given for advanced disease.
Immunotherapy in the form of immune checkpoint inhibitors may be part of your treatment plan if you have a certain type of recurrent or metastatic sinus and nasal cancer. The doctor will test for the tumor’s PD-L1 expression, which may indicate whether the tumor could respond to immunotherapy. If expression is more than 1 percent, the tumor is considered to be PD-L1 positive and immunotherapy alone may be used. If PD-L1 is negative, immunotherapy and traditional chemotherapy are often combined for recurrent or metastatic cancer.
Targeted therapy may be an option to treat certain types of sinus and nasal cancer. Targeted therapy in the form of epidermal growth factor receptor (EGFR) inhibitors may be used in combination with radiation therapy. Targeted therapy drugs may be used with or without chemotherapy and after surgery for advanced cancers.
TNM Classification for Sinus and Nasal Cancer
| Classification | Definition |
| Tumor (T) | |
| TX | Primary tumor cannot be assessed. |
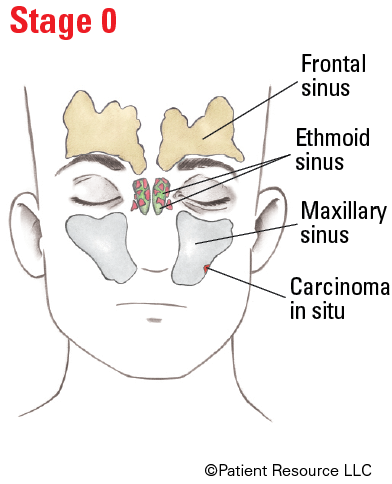
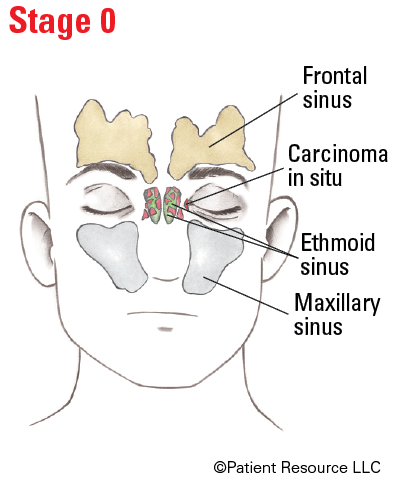
| Tis | Carcinoma in situ. |
| Maxillary Sinus | |
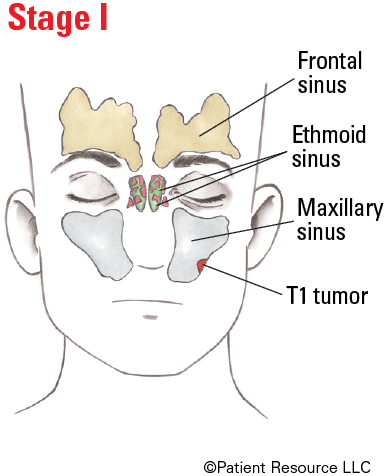
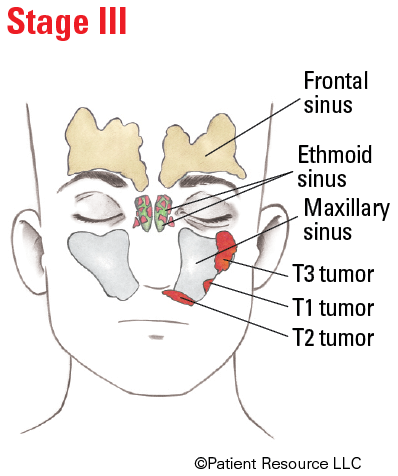
| T1 | Tumor limited to maxillary sinus mucosa with no erosion or destruction of bone. |
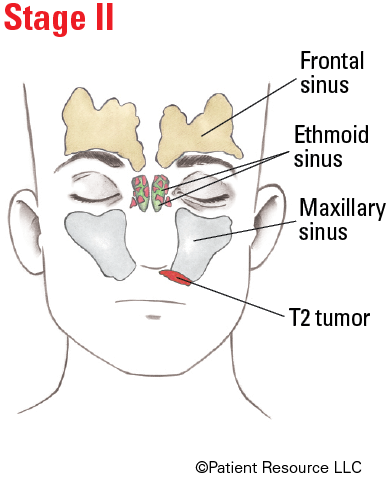
| T2 | Tumor causing bone erosion or destruction including extension into the hard palate and/or middle nasal meatus, except extension to posterior wall of maxillary sinus and pterygoid plates. |
| T3 | Tumor invades any of the following: bone of the posterior wall of maxillary sinus, subcutaneous tissues, floor or medial wall of orbit (eye socket), pterygoid fossa, ethmoid sinuses. |
| T4 | Moderately advanced or very advanced local disease. |
| T4a |
Moderately advanced local disease.
Tumor invades anterior orbital contents (eye socket), skin of cheek, pterygoid plates, infratemporal fossa, cribriform plate, sphenoid or frontal sinuses. |
| T4b |
Very advanced local disease.
Tumor invades any of the following: orbital apex (eye socket), dura (membrane surrounding the brain and spinal cord), brain, middle cranial fossa, cranial nerves other than maxillary division of trigeminal nerve (V2), nasopharynx (upper part of throat) or clivus (bony base of skull). |
| Nasal Cavity and Ethmoid Sinus | |
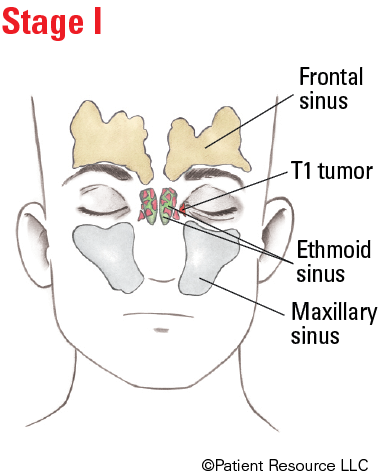
| T1 | Tumor restricted to any one subsite, with or without bony invasion. |
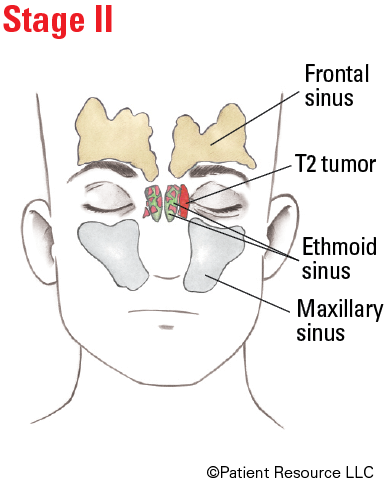
| T2 | Tumor invading two subsites in a single region or extending to involve an adjacent region within the nasoethmoidal complex, with or without bony invasion. |
| T3 | Tumor extends to invade the medial wall or floor of the orbit (eye socket), maxillary sinus, palate, or cribriform plate. |
| T4 | Moderately advanced or very advanced local disease. |
| T4a |
Moderately advanced local disease.
Tumor invades any of the following: anterior orbital contents (eye socket), skin of nose or cheek, minimal extension to anterior cranial fossa, pterygoid plates, sphenoid or frontal sinuses. |
| T4b |
Very advanced local disease.
Tumor invades any of the following: orbital apex (eye socket), dura (membrane surrounding the brain and spinal cord), brain, middle cranial fossa, cranial nerves other than (V2), nasopharynx (upper part of throat) or clivus (bony base of skull). |
| Node (N) | |
| NX | Regional lymph nodes cannot be assessed. |
| N0 | No regional lymph node metastasis. |
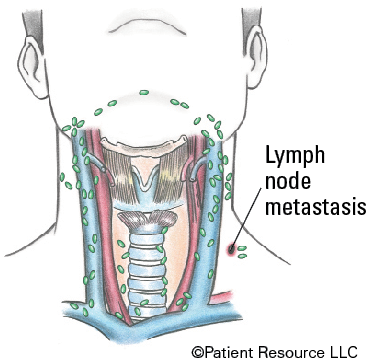
| N1 | Metastasis in a single ipsilateral (on the same side) lymph node 3 cm or smaller in greatest dimension and ENE*(-). |
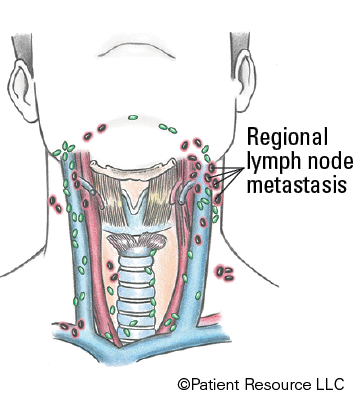
| N2 |
Metastasis in a single ipsilateral (on the same side) lymph node 3 cm or smaller in greatest dimension and ENE*(+);
or larger than 3 cm but not larger than 6 cm in greatest dimension and ENE(-); or metastases in multiple ipsilateral lymph nodes, none larger than 6 cm in greatest dimension and ENE(-); or in bilateral (on both sides) or contralateral (on the opposite side) lymph node(s), none larger than 6 cm in greatest dimension and ENE(-). |
| N2a |
Metastasis in single ipsilateral (on the same side) node 3 cm or smaller in greatest dimension and ENE*(+);
or a single ipsilateral node larger than 3 cm but not larger than 6 cm in greatest dimension and ENE(-). |
| N2b | Metastases in multiple ipsilateral (on the same side) nodes none larger than 6 cm in greatest dimension and ENE*(-). |
| N2c | Metastases in bilateral (on both sides) or contralateral (on the opposite side) lymph node(s), none larger than 6 cm in greatest dimension and ENE*(-). |
| N3 |
Metastasis in a lymph node larger than 6 cm in greatest dimension and ENE*(-);
or metastasis in a single ipsilateral (on the same side) node larger than 3 cm in greatest dimension and ENE(+); or multiple ipsilateral, contralateral (on the opposite side) or bilateral (on both sides) nodes, any with ENE(+); or a single contralateral node of any size and ENE(+). |
| N3a | Metastasis in a lymph node larger than 6 cm in greatest dimension and ENE*(-). |
| N3b |
Metastasis in a single ipsilateral (on the same side) node larger than 3 cm in greatest dimension and ENE*(+);
or multiple ipsilateral, contralateral (on the opposite side) or bilateral (on both sides) nodes, any with ENE(+); or a single contralateral node of any size and ENE(+). |
| >Metastasis (M) | |
| M0 | No distant metastasis. |
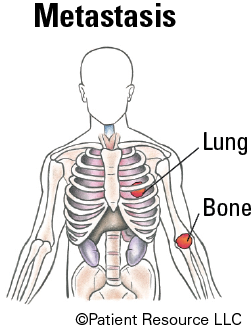
| M1 | Distant metastasis. |
Staging Sinus and Nasal Cancer
| Stage | T | N | M |
| 0 | Tis | N0 | M0 |
| I | T1 | N0 | M0 |
| II | T2 | N0 | M0 |
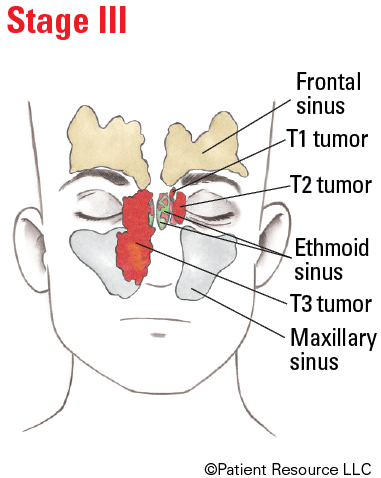
| III |
T3
T1, T2, T3 |
N0
N1 |
M0
M0 |
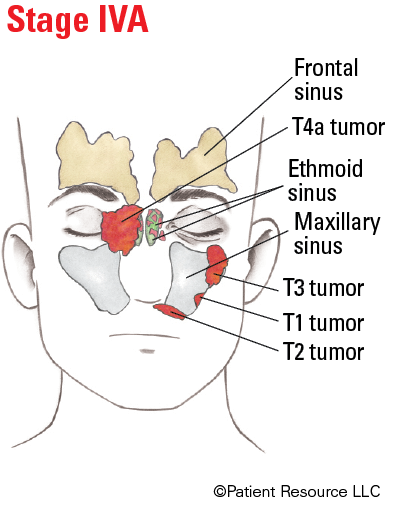
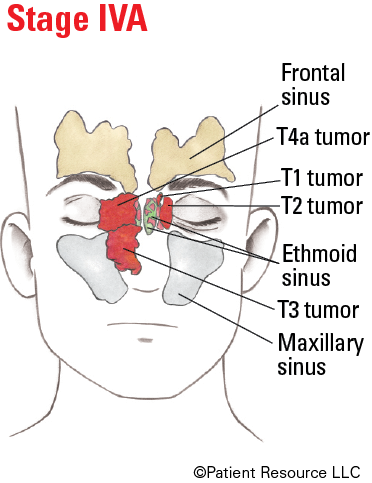
| IVA |
T4a
T1, T2, T3, T4a |
N0, N1
N2 |
M0
M0 |
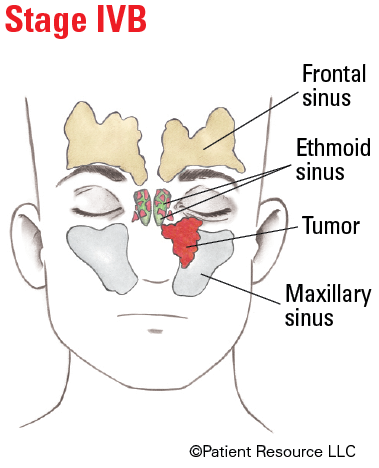
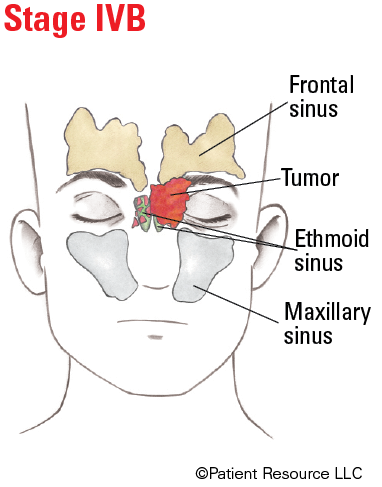
| IVB |
Any T
T4b |
N3
Any N |
M0
M0 |
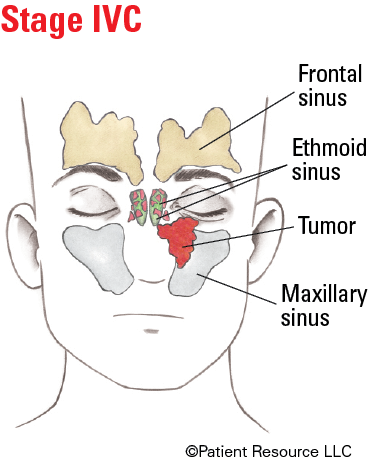
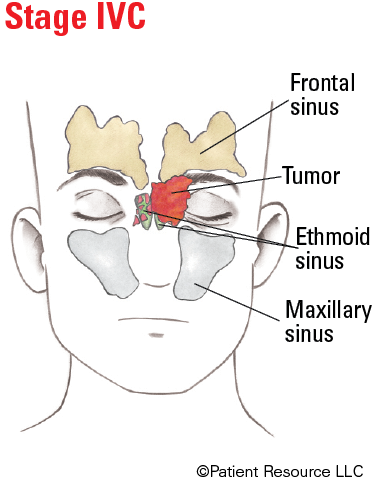
| IVC | Any T | Any N | M1 |
Illustrated Stages of Sinus and Nasal Cancer (Ethmoid)
Illustrated Stages of Sinus and Nasal Cancer (Maxillary)