Melanoma
Staging
Your doctor will order a variety of tests to diagnose and learn about the melanoma. The diagnostic tests provide information about the tumor’s location and size, whether it has spread to lymph nodes or other organs, any biomarkers and the type or subtype of the cancer.
This information will be documented in a pathology report, which includes a description of cells and tissues made by a pathologist based on microscopic evidence. The results allow your doctor to stage your cancer. Staging provides essential information to your medical team. It defines the extent of the disease and helps the team predict outcomes (prognosis, or chance of recovery) as well as determine the best treatment plan for you.
Melanoma is usually staged twice. First, your doctor considers the results of your physical exam and skin biopsy to assign a clinical stage. During a more extensive procedure, the lesion (or as much of it as possible) is removed along with some healthy tissue surrounding it. In a different procedure, some lymph nodes may be removed (see Sentinel Lymph Node Mapping, page 6). After reviewing these specimens with and without a microscope and noting key characteristics, a pathologist also considers results from lymph node biopsies and other tissue that was examined. Then a pathologic stage is assigned. Because the pathologic stage is based on more details about the melanoma, this staging is the most accurate and is important in determining appropriate treatment options for your diagnosis.
Both the clinical and pathologic stages of melanoma are classified according to the tumor, node, metastasis (TNM) system developed by the American Joint Committee on Cancer (AJCC). This system uses the size and extent of the tumor (T), whether cancer cells are found in nearby lymph nodes (N) and whether the cancer has metastasized, or spread, to other parts of the body (M). The thickness of the primary melanoma is used to classify the melanoma in the T category. Additionally, each T classification is further divided into groups according to whether ulceration (a break in the outer layer of skin over the melanoma) is absent or present. The node (N) classification is used to describe how many lymph nodes contain melanoma cells.
Be aware that the stage of your cancer may change. If your cancer returns after treatment, diagnostic tests may be repeated to reassess your stage. This is known as restaging. If a new stage is assigned, it is often preceded by an “r” to denote that it has been restaged.
Table 1 - AJCC TNM System for Classifying Melanoma of the skin
| Classification | Definition | |
| Tumor (T) | ||
| T Category | Thickness | Ulceration Status |
| TX | Primary tumor cannot be assessed | Not applicable |
| T0 | There is no evidence of primary tumor | Not applicable |
| Tis | Melanoma in situ | Not applicable |
| T1 | ≤ (not more than) 1.0 mm. | Unknown or unspecified |
| T1a | < (less than) 0.8 mm. | Without ulceration |
| T1b |
< (less than) 0.8 mm.
< 0.8 – 1.0 mm. |
With ulceration
With or without ulceration |
| T2 | > (more than) 1.0 – 2.0 mm. | Unknown or unspecified |
| T2a | > (more than) 1.0 – 2.0 mm. | Without ulceration |
| T2b | > (more than) 1.0 – 2.0 mm. | With ulceration |
| T3 | > (more than) 2.0 – 4.0 mm. | Unknown or unspecified |
| T3a | > (more than) 2.0 – 4.0 mm. | Without ulceration |
| T3b | > (more than) 2.0 – 4.0 mm. | With ulceration |
| T4 | > (more than) 4.0 mm. | Unknown or unspecified |
| T4a | > (more than) 4.0 mm. | Without ulceration |
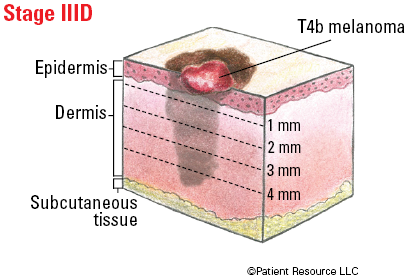
| T4b | > (more than) 4.0 mm. | With ulceration |
| Node (N) | ||
| N Category | Number of tumor-involved regional lymph nodes | Metastases status* |
| NX | Regional nodes not assessed. | No |
| N0 | No regional metastases detected. | No |
| N1 | One tumor-involved node or in-transit, satellite, and/or microsatellite metastases with no tumor-involved nodes. | |
| N1a | One clinically occult. | No |
| N1b | One clinically detected. | No |
| N1c | No regional lymph node disease. | Yes |
| N2 | Two or three tumor-involved nodes or in-transit, satellite, and/or microsatellite metastases with one tumor-involved node. | |
| N2a | Two or three clinically occult. | No |
| N2b | Two or three, at least one of which was clinically detected. | No |
| N2c | One clinically occult or clinically detected. | Yes |
| N3 | Four or more tumor-involved nodes or in-transit, satellite, and/or microsatellite metastases with two or more tumor-involved nodes, or any number of matted nodes without or with in-transit, satellite, and/or microsatellite metastases. | |
| N3a | Four or more clinically occult. | No |
| N3b | Four or more, at least one of which was clinically detected, or presence of any number of matted nodes. | No |
| N3c | Two or more clinically occult or clinically detected and/or presence of any number of matted nodes. | Yes |
| * In-transit metastases occur more than 2 cm from the primary melanoma (both on the surface of the skin or below the surface of the skin) to the regional lymph nodes. Satellite metastases occur on or below the skin within 2 cm of the primary melanoma. Microsatellite metastases in the skin or in the deeper layer of the dermis near or deep within the skin of the primary melanoma is detected upon microscopic examination. | ||
| Metastasis (M) | ||
| M Category* | Anatomic site | LDH level |
| M0 | No evidence of distant metastasis. | Not applicable |
| M1 | Evidence of distant metastasis. | See below |
| M1a | Distant metastasis to skin, soft tissue including muscle, and/or nonregional lymph node. | Not recorded or unspecified |
| M1a(0) | Not elevated | |
| M1a(1) | Elevated | |
| M1b | Distant metastasis to lung with or without M1a sites of disease. | Not recorded or unspecified |
| M1b(0) | Not elevated | |
| M1b(1) | Elevated | |
| M1c | Distant metastasis to non-CNS visceral sites with or without M1a or M1b sites of disease. | Not recorded or unspecified |
| M1c(0) | Not elevated | |
| M1c(1) | Elevated | |
| M1d | Distant metastasis to CNS with or without M1a, M1b, or M1c sites of disease. | Not recorded or unspecified |
| M1d(0) | Normal | |
| M1d(1) | Elevated | |
| *Suffixes for M category: (0) LDH not elevated, (1) LDH elevated. No suffix is used if LDH is not recorded or is unspecified. | ||
Table 2 - Stages of Melanoma of the Skin
| Stage | T | N | M |
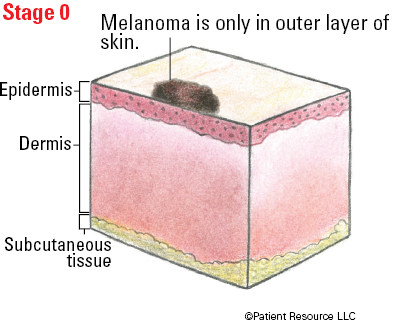
| 0 | Tis | N0 | M0 |
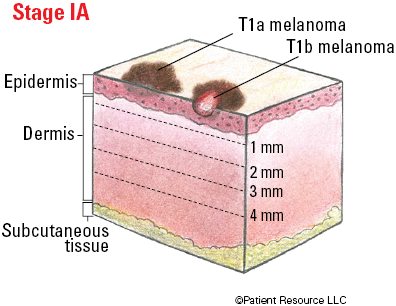
| IA |
T1a
T1b |
N0
N0 |
M0
M0 |
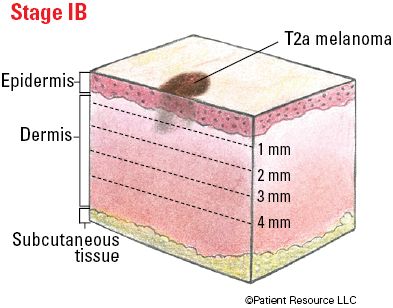
| IB | T2a | N0 | M0 |
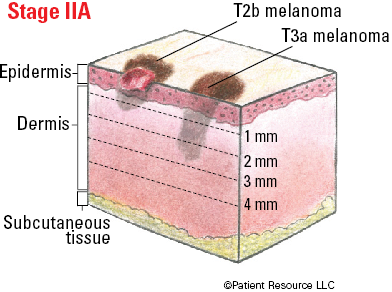
| IIA |
T2b
T3a |
N0
N0 |
M0
M0 |
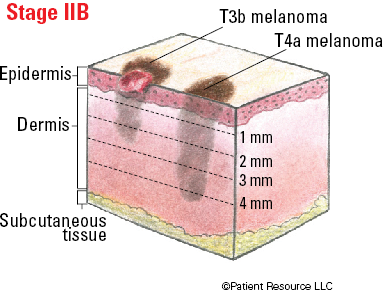
| IIB |
T3b
T4a |
N0
N0 |
M0
M0 |
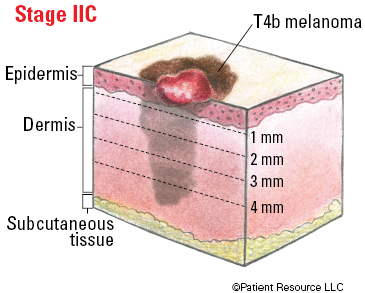
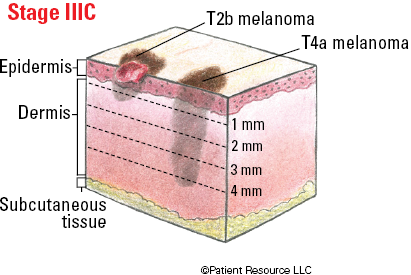
| IIC | T4b | N0 | M0 |
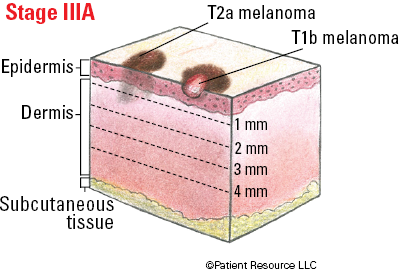
| IIIA | T1a/b-T2a | N1a or N2a | M0 |
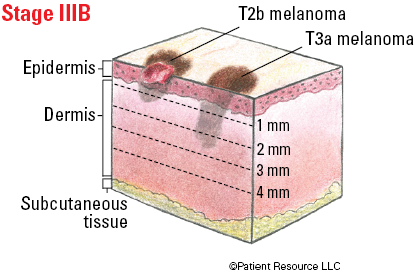
| IIIB |
T0
T1a/b-T2a T2b/T3a |
N1b, N1c
N1b/c or N2b N1a-N2b |
M0
M0 M0 |
| IIIC |
T0
T1a-T3a T2b/T4a T4b |
N2b, N2c, N3b or N3c
N2c or N3a/b/c Any N ≥ N1 N1a-N2c |
M0
M0 M0 M0 |
| IIID | Any T, Tis | Any N | M0 |
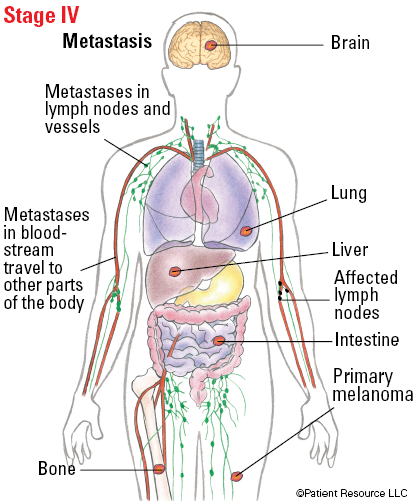
| IV | Any T, Tis | Any N | M1 |
Understanding Pathology Terms
The results of the diagnostic tests are included in a pathology report that your doctor can share with you. Learning these terms will help you understand your stage of melanoma.
Location: where the tumor is found
Thickness: how deep the tumor has grown into the skin
Mitotic rate: a measure of how fast cancer cells are dividing and growing
Ulceration status: a microscopic evaluation to determine whether the tumor’s top skin layer over the melanoma is present and intact (not ulcerated) or broken or missing (ulcerated)
Dermal mitotic rate: how many melanoma cells are actively growing and dividing
Peripheral margin status: the presence or absence of cancer cells in the normal-looking tissue that was removed from around the tumor
Deep margin status: the presence or absence of cancer cells in the normal-looking tissue that was removed from underneath the tumor
Microsatellitosis: the presence of tiny satellite tumors in the lymphatic channels that have spread to skin near the first melanoma tumor that can only be seen with a microscope
Vertical growth phase: evidence of tumor growth deeper into the skin
Angiolymphatic invasion: melanoma cells have grown into blood or lymph vessels
Neurotropism: the presence of melanoma cells in or around the nerves in the skin
Illustrated Stages of Melanoma of the Skin