

Cervical Cancer
Overview and Staging
Now that you have received a cervical cancer diagnosis, take a breath and try to digest all the information you’ve been given. Empower yourself by learning about your specific diagnosis and treatment options so you can make informed decisions throughout your cancer care. It will be important for you to speak up and let your medical team know your preferences. By becoming an active partner on your health care team, you will all be immeasurably stronger and more effective.
Though a cervical cancer diagnosis can feel isolating, you are not alone. You will be surrounded by medical professionals, advocacy groups, survivors and others who have been affected by cervical cancer. Do not hesitate to ask your health care team for a referral to support groups or mental health professionals to assist you as you come to terms with the diagnosis.
Cervical Cancer Basics
Cervical cancer develops in the cervix, which is the lower, narrow end of the uterus that leads to the vagina (see Figure 1). Before cancer develops, changes in normal cells create benign abnormalities (not cancerous) that can develop over time into cancer. Cervical cancer is typically slow-growing and usually found at an early stage because of routine HPV screening and the Papanicolaou (Pap) test (see Understanding HPV, page 5). Pap tests, which are done during a pelvic exam, look for any abnormal cell changes on the cervix that could become cancerous.
Abnormal cells found on the surface of the cervix are often referred to as dysplasia. Cervical intraepithelial neoplasia (CIN) is dysplasia discovered by biopsy. If left untreated, dysplasia can become severe and may develop into carcinoma in situ, the most advanced form of a premalignancy. Invasive cervical cancer typically develops from these precancerous conditions.
The human papillomavirus (HPV) is a major risk factor and almost always the cause of cervical cancer. HPV is a common sexually transmitted viral infection with more than 200 different subtypes. Those most likely to cause cervical cancer are called high-risk and can lead to the abnormal cell changes that may develop into cancer. Risk factors associated with HPV may include any sexual activity that exposes a person to the virus (even with just one partner), long-term use of oral contraceptives, multiple full-term pregnancies, a weakened immune system (decreasing the ability to fight off an HPV infection) and tobacco use. Not all women infected with HPV will develop cervical cancer because the body’s immune system often resolves the infection on its own.
Staging
Determining the type of cervical cancer you have and its extent will be your doctor’s first priority. Once a diagnosis is made, your doctor will classify and stage the cancer according to the TNM system developed by the American Joint Committee on Cancer (AJCC). This system classifies the cancer by tumor (T), node (N) and metastasis (M). The T category describes the size and location of the primary tumor. The N category indicates whether the lymph nodes show evidence of cancer cells. The number and location of these lymph nodes are important because they show how far the disease has spread. The M category describes metastasis (spread of cancer to another part of the body), if any. Once the cancer is classified, an overall stage is assigned (see Tables 1 and 2).
Your doctor will use the information about your type and stage of cervical cancer to choose the best treatment option for you. Treatments for cervical cancer may include a combination of surgery, radiation therapy or drug therapy. You might also receive palliative (supportive) therapy to relieve the symptoms and side effects you may experience.
Consider a Second Opinion
Once you receive a cervical cancer diagnosis, you are encouraged to see a doctor or cancer center with experience treating cervical cancer. Do not hesitate to ask your doctor for guidance in obtaining a referral.
Seeking a second opinion is recommended for multiple reasons. Doctors bring different training and experience to treatment planning. Some doctors may favor one treatment approach, such as a clinical trial, while others might suggest a different combination of treatments. Another doctor’s opinion may change the diagnosis or reveal a treatment of which your first doctor was not aware. You need to hear reasons and recommendations that include all your treatment options. A second opinion is also a way to make sure your pathology diagnosis and staging are accurate.
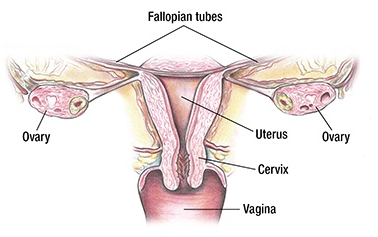
Table 1. TNM Cervical Cancer Classifications
| Classification | Definition |
| Tumor (T) | |
| TX | Primary tumor cannot be assessed. |
| T0 | No evidence of primary tumor. |
| T1 | Carcinoma is strictly confined to the cervix (extension to the corpus should be disregarded). |
| T1a | Invasive carcinoma that can be diagnosed only by microscopy with maximum depth of not more than 5.0 mm. |
| T1a1 | Measured stromal invasion of not more than 3 mm in depth. |
| T1a2 | Measured stromal invasion of more than 3 mm and not more than 5 mm. |
| T1b | Invasive carcinoma with measured deepest invasion of more than 5 mm (greater than Stage IA); lesion limited to the cervix uteri with size measured by maximum tumor diameter. Note: The involvement of vascular/lymphatic spaces should not change the staging. The lateral extent of the lesion is no longer considered. |
| T1b1 | Invasive carcinoma of more than 5 mm depth of stromal invasion and not more than 2 cm in greatest dimension. |
| T1b2 | Invasive carcinoma of more than 2 cm and not more than 4 cm in greatest dimension. |
| T1b3 | Invasive carcinoma of more than 4 cm in greatest dimension. |
| T2 | Carcinoma invades beyond the uterus but has not extended onto the lower third of the vagina or to the pelvic wall. |
| T2a | Involvement limited to the upper two-thirds of the vagina without parametrial invasion. |
| T2a1 | Invasive carcinoma of not more than 4 cm in greatest dimension. |
| T2a2 | Invasive carcinoma of more than 4 cm in greatest dimension. |
| T2b | With parametrial invasion but not up to the pelvic wall. |
| T3 | Carcinoma involves the lower third of the vagina and/or extends to the pelvic wall and/or causes hydroephrosis or nonfunctioning kidney. Note: The pelvic wall is defined as the muscle, fascia, neurovascular structures and skeletal portions of the bony pelvis. Cases with non cancer-free space between the tumor and pelvic wall by rectal examination are FIGO III. |
| T3a | Carcinoma involves the lower third of the vagina, with no extension to the pelvic wall. |
| T3b | Extension to the pelvic wall and/or hydronephrosis or nonfunctioning kidney (unless known to be due to another cause). |
| T4 | Carcinoma has involved (biopsy-proven) the mucuosa of the bladder or rectum or has spread to adjacent organs. Bullous edema, such, does not permit a case to be assigned to stage IVA.extending beyond the true pelvis. |
| Node (N) | |
| Nx | Regional lymph nodes cannot be assessed. |
| N0 | No regional lymph node metastasis. |
| N0(i+) | Isolated tumor cells in regional lymph node(s) no greater than 0.2 mm, or single cells or clusters of cells not more than 200 cells in a single lymph node cross section. |
| N1 | Regional lymph node metastasis to pelvic lymph nodes only. |
| N1mi | Regional lymph node metastasis (greater than 0.2 mm but not more than 2.0 mm in diameter) to pelvic lymph nodes. |
| N1a | Regional lymph node metastasis (greater than 2.0 mm in diameter) to pelvic lymph nodes. |
| N2 | Regional lymph node metastasis to para-aortic lymph nodes with or without positive pelvic lymph nodes. |
| N2mi | Regional lymph node metastasis (greater than 0.2 but not more than 2.0 mm in diameter) to para-aortic lymph nodes, with or without positive pelvic lymph nodes. |
| N2a | Regional lymph node metastasis (greater than 2.0 in diameter) to para-aortic lymph nodes, with or without positive pelvic lymph nodes. |
| Metastasis (M) | |
| M0 | No distant metastasis. |
| cM1 | Distant metastasis (including metastasis to inguinal (groin) lymph nodes, intraperitoneal disease, lung, liver or bone) (excludes metastasis to pelvic or para-aortic lymph nodes or vagina. |
| pM1 | Microscopic confirmation of distant metastasis (includes metastasis to inguinal (groin) lymph nodes, intraperitoneal disease, lung, liver or bone) (excludes metastasis to pelvic or para-aortic lymph nodes or vagina). |
Table 2. Stages of Cervical Cancer
| Stage | TNM Classification |
| I | T1, N0, M0 |
| IA | T1a, N0, M0 |
| IA1 | T1a1, N0, M0 |
| IA2 | T1a2, N0, M0 |
| IB | T1b, N0, M0 |
| IB1 | T1b1, N0, M0 |
| IB2 | T1b2, N0, M0 |
| IB3 | T1b3, N0, M0 |
| II | T2, N0, M0 |
| IIA | T2a, N0, M0 |
| IIA1 | T2a1, N0, M0 |
| IIA2 | T2a2, N0, M0 |
| IIB | T2b, N0, M0 |
| III | T3, N0, M0 |
| IIIA | T3a, N0, M0 |
| IIIB | T3b, N0, M0 |
| IIIC1 | TX, T0, T1-3, N1, M0 |
| IIIC2 | TX, T0, T1-3, N2, M0 |
| IVA | T4, Any N, M0 |
| IVB | Any T, Any N, M1 |
