Skin Cancers
Staging
Determining the type of skin cancer you have and its extent will be your doctor’s main priority. This information is used to create a treatment plan designed for you. First, your doctor will start with diagnostic tests to learn as much as possible about your cancer and determine how to stage it.
These tests will include a complete medical history, a physical exam and a skin biopsy (see page 4). This information will be documented in a pathology report along with a description of cells and tissues made by the pathologist examining a biopsy sample. Sometimes, imaging tests are also performed.
Initial tests will also determine whether your skin cancer is cutaneous squamous cell carcinoma (cSCC), basal cell carcinoma (BCC) or Merkel cell carcinoma (MCC). This is important because knowing the type of cell in which the cancer started in helps your doctor stage and better treat your cancer. Understanding the cancer’s stage is also critical to identifying clinical trials that may be appropriate for your treatment plan.
The Staging Process
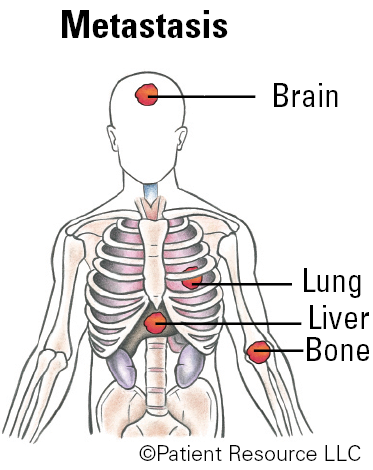
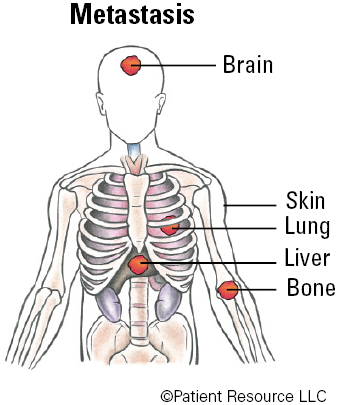
Non-melanoma skin cancers are staged using the TNM system developed by the American Joint Committee on Cancer (AJCC). This system classifies the cancer by tumor (T), node (N) and metastasis (M). The T category describes the size and location of the primary tumor in the skin. The N category indicates whether the lymph nodes show evidence of cancer cells. The number and location of these lymph nodes are important because they show how far the disease has spread. The M category describes metastasis (spread of cancer to another part of the body), if any. Once the cancer is classified, an overall stage is assigned.
All three skin cancers are staged with AJCC, but cSCC and BCC include a risk classification, which defines the likelihood that they will return. That risk is determined from the information on the pathology report and will be considered as your doctor determines treatment for cSCC or BCC.
The risk groups for cSCC have three categories:
- Low-risk cSCC does not have any of the features in the high-risk and very high-risk categories.
- High-risk cSCC has an increased risk of coming back but does not have any of the characteristics of very high-risk cSCC. For this category, the tumor is more than 2 cm but no more than 4 cm across, it is a recurrent tumor that has been treated once before, it grows quickly, it is in a location that is a chronic wound or was previously treated with radiation, it is 2 to 6 mm deep or cancer cells have invaded small nerves in or near the tumor. cSCC tumors on the lip or ear are also considered high-risk as they have a higher chance of spreading compared to tumors on other sites.
- Very high-risk cSCC has an increased risk of returning and spreading to other parts of the body. It is at least 4 cm across, the cells look abnormal under a microscope, the tumor is more than 6 mm deep, has grown beyond the fat layer, or has invaded a blood vessel or lymph vessel near the tumor.
Following are the risk groups for BCC:
- list item
- list item
- list item
- Low-risk BCC is small and superficial, less than 2 cm, has a clear, defined edge and has not been treated before.
- High-risk BCC has a higher chance of returning after treatment. It is usually found on areas of the face, head, neck, arms, hands, trunk, legs, feet and sometimes the genital area. It can be 2 cm or larger, has a poorly defined edge, has previously come back after treatment or shows an aggressive growth pattern under the microscope.
- Advanced disease means the BCC has spread to the surrounding area, to the lymph nodes or to distant areas of the body.
Be aware that the stage of your cancer may change. If your cancer returns after treatment, diagnostic tests may be repeated to reassess the stage, and your treatment plan may be revised.
Treatments may include a combination of surgery, radiation therapy or drug therapy. You might also receive palliative (supportive) therapy to relieve the symptoms and side effects.
Your Pathology Report
Pathology is the study of diseases and how they affect the body’s cells and tissues. A pathologist is a doctor who is specially trained to identify diseases by studying cells and tissues under a microscope and recording the findings in a pathology report.
A pathologist will examine the specimen with and without a microscope, documenting its size, describing its appearance and determining its characteristics. The goal is to identify all of the tumor’s characteristics. Therefore, the accuracy of testing and interpretation is essential because treatment is planned according to the final results. The final diagnosis is based on all the findings of the examination and is included in your pathology report.
Pathology reports will vary in appearance and content at different cancer centers and hospitals, but most of them include the same information.
Results are most likely returned between one and two weeks, but some tests may take longer than others and may be performed in a different hospital than where you may be treated.
Talk with your doctor about when and how you will receive results to reduce the anxiety that can occur before, during or after a medical scan or test. You can ask your doctor for a copy of the pathology report. In some cases, you may ask to discuss the report with the pathologist.
Consider Getting a Second Opinion
Once you receive a skin cancer diagnosis, you are encouraged to see a doctor or cancer center with experience treating skin cancer. Do not hesitate to ask your doctor for guidance in obtaining a referral or a second opinion.
Seeking a second opinion is recommended for multiple reasons. Doctors bring different training and experience to treatment planning. Some doctors may favor one treatment approach, such as a clinical trial, while others might suggest a different combination of treatments. Another doctor’s opinion may change the diagnosis or reveal a treatment your first doctor was not aware of or did not suggest. You need to hear reasons and recommendations that include all your treatment options. A second opinion is also a way to make sure your pathology diagnosis and staging are accurate and can be a resource for any additional questions.
AJCC TNM System for Classifying BCC & cSCC
| Classification | Definition |
| Tumor (T) | |
| Tx | Primary tumor cannot be assessed. |
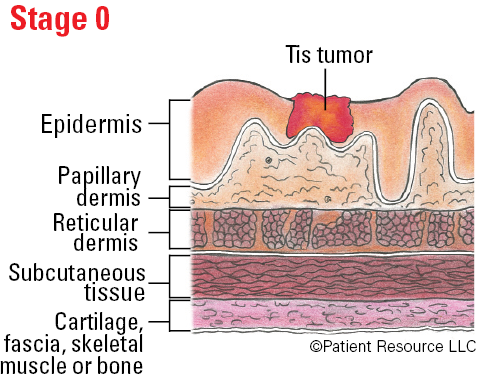
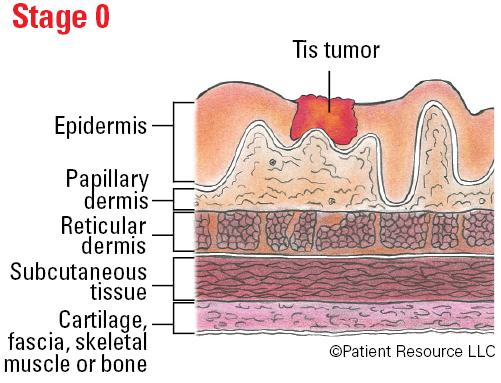
| Tis | Carcinoma in situ. |
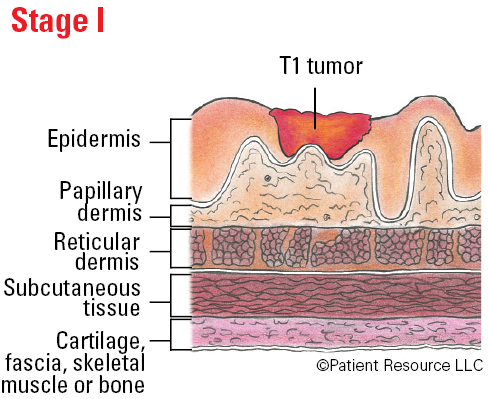
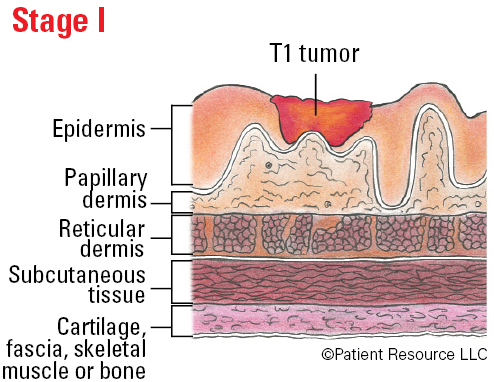
| T1 | Tumor smaller than 2 cm in greatest dimension. |
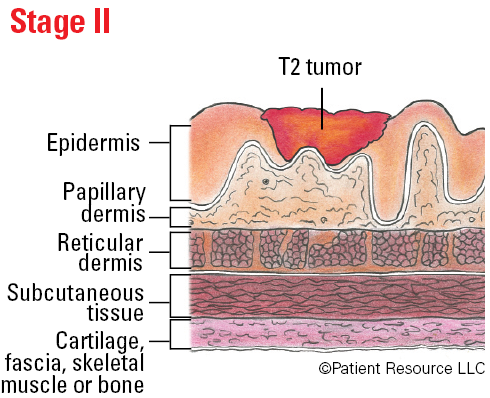
| T2 | Tumor 2 cm or larger, but smaller than 4 cm in greatest dimension. |
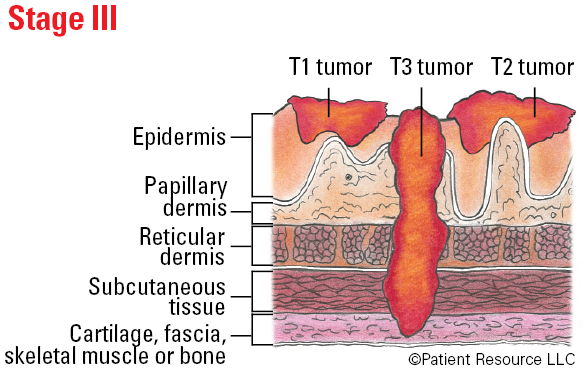
| T3 | Tumor 4 cm or larger in maximum dimension or minor bone erosion or perineural invasion or deep invasion. |
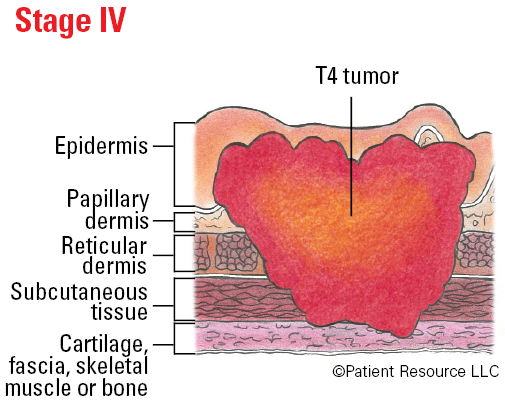
| T4 | Tumor with gross cortical bone/marrow, skull base invasion and/or skull base foramen invasion. |
| T4a | Tumor with gross cortical bone/marrow invasion. |
| T4b | Tumor with skull base invasion and/or skull base foramen involvement. |
| Node (N) | |
| Nx | Regional lymph nodes cannot be assessed. |
| N0 | No regional lymph node metastasis. |
| N1 |
Metastasis in a single ipsilateral lymph node, 3 cm or smaller in greatest dimension and ENE**(+);
or larger than 3 cm but not larger than 6 cm in greatest dimension and ENE(–); or metastases in multiple ipsilateral (on the same side of the body) lymph nodes, none larger than 6 cm in greatest dimension and ENE(–); or in bilateral (on both sides of the body) or contralateral (on the opposite side of the body) lymph node(s), none larger than 6 cm in greatest dimension, ENE(–). |
| N2a |
Metastasis in single ipsilateral (on the same side of the body) node 3 cm or smaller in greatest dimension and ENE**(+);
or a single ipsilateral node larger than 3 cm but not larger than 6 cm in greatest dimension and ENE(–). |
| N2b | Metastasis in multiple ipsilateral (on the same side of the body) nodes, none larger than 6 cm in greatest dimension and ENE**(–). |
| N2c | Metastasis in bilateral (on both sides of the body) or contralateral (on the opposite side of the body) lymph node(s), none larger than 6 cm in greatest dimension and ENE(–). |
|
N3
|
Metastasis in a lymph node larger than 6 cm in greatest dimension and ENE**(–);
or in a single ipsilateral (on the same side of the body) node larger than 3 cm in greatest dimension and ENE(+); or multiple ipsilateral, contralateral (on the opposite side of the body), or bilateral (on both sides of the body) nodes, any with ENE(+); or a single contralateral (on the opposite side of the body) node 3 cm or smaller and ENE(+). |
| N3a | Metastasis in a lymph node larger than 6 cm in greatest dimension and ENE**(–). |
| N3b |
Metastasis in a single ipsilateral (on the same side of the body) node larger than 3 cm in greatest dimension and ENE**(+);
or multiple ipsilateral, contralateral (on the opposite side of the body), or bilateral (on both sides of the body) nodes, any with ENE(+); or a single contralateral (on the opposite side of the body) node 3 cm or smaller and ENE(+). |
|
Note: A designation of “U” or “L” may be used for any N category to indicate metastasis above the lower border of the cricoid (U) or below the lower border of the cricoid (L).
**Extranodal extension (ENE) refers to cancer cells that have spread through the node into surrounding connective tissue. |
|
| Metastasis (M) | |
| M0 | No distant metastasis. |
| M1 | Distant metastasis. |
Stages of Non-Melanoma Skin Cancer
| Stage | T | N | M |
| 0 | Tis | N0 | M0 |
| I | T1 | N0 | M0 |
| II | T2 | N0 | M0 |
| III |
T3
T1 - T3 |
N0
N0 |
M0
M0 |
| IV |
T1-T3
Any T T4 Anyh T |
N2
N3 Any N Any N |
M0
M0 M0 M1 |
Stages of Non-Melanoma Skin Cancer
| Classification | Definition |
| GX | Grade cannot be assessed. |
| G1 | Well differentiated. |
| G2 | Moderately differentiated. |
| G3 | Poorly differentiated. |
| G4 | Undifferentiated. |
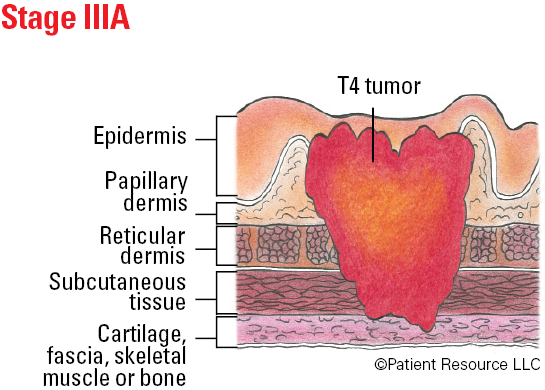
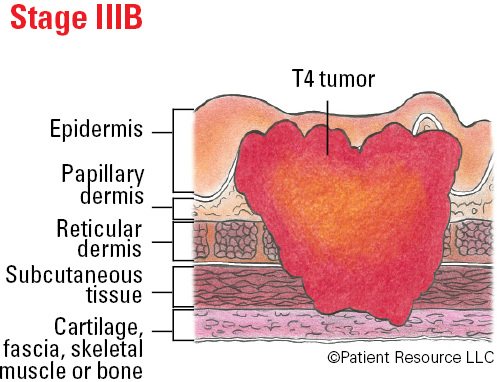
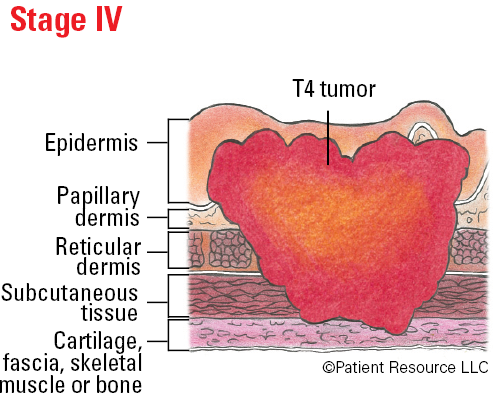
Illustrated Stages of Non-Melanoma Skin Cancer
AJCC TNM System for Classifying Merkel Cell Carcinoma (MCC)
| Classification | Definition |
| Tumor (T) | |
| Tx | Primary tumor cannot be assessed (e.g., curetted). |
| T0 | No evidence of primary tumor. |
| Tis | In situ primary tumor. |
| T1 | Maximum clinical tumor diameter < 2 cm (or less). |
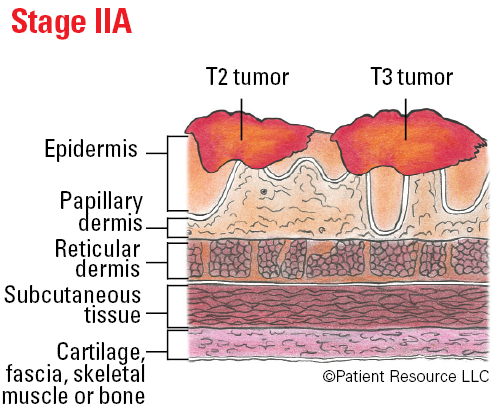
| T2 | Maximum clinical tumor diameter > (more than) 2 cm but ≯ (not more than) 5 cm. |
| T3 | Maximum clinical tumor diameter > (more than) 5 cm. |
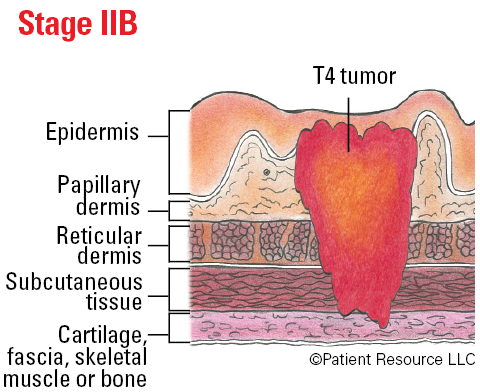
| T4 | Primary tumor invades fascia, muscle, cartilage, or bone. |
| Node (N) | |
| Nx | Regional lymph nodes cannot be assessed. |
| N0 | No regional lymph node metastasis detected on pathological evaluation. |
| N1 | Metastasis in regional lymph node(s). |
| N1a(sn) | Clinically occult regional lymph node metastasis identified only by sentinel lymph node biopsy. |
| N1a | Clinically occult regional lymph node metastasis following lymph node dissection. |
| N1b | Clinically and/or radiologically detected regional lymph node metastasis, microscopically confirmed. |
| N2 | In-transit metastasis (discontinuous from primary tumor; located between primary tumor and draining regional nodal basin, or distal to the primary tumor) without lymph node metastasis. |
| N3 | In-transit metastasis (discontinuous from primary tumor; located between primary tumor and draining regional nodal basin, or distal to the primary tumor) with lymph node metastasis. |
| Metastasis (M) | |
| M0 | No distant metastasis detected on clinical and/or radiologic examination. |
| M1 | Distant metastasis microscopically confirmed. |
| M1a | Metastasis to distant skin, distant subcutaneous tissue, or distant lymph node(s), microscopically confirmed. |
| M1b | Metastasis to lung, microscopically confirmed. |
| M1c | Metastasis to all other distant sites, microscopically confirmed. |
Stages of Merkel Cell Carcinoma (MCC)
| Stage | T | N | M |
| 0 | Tis | N0 | M0 |
| I | T1 | N0 | M0 |
| IIA | T2-3 | N0 | |
| IIB | T4 | N0 | M0 |
| IIIA |
T1-4
T0 |
N1a(sn) or
N1a N1b |
M0
M0 |
| IIIB | T1-4 | N1b-3 | M0 |
| IV | T0-4 | Any N | M1 |
Illustrated Stages of Merkel Cell Carcinoma (MCC)