

Skin Cancers
Treatment Planning for Cutaneous Squamous Cell Carcinoma
Cutaneous squamous cell carcinoma (cSCC) develops in squamous cells, which form in the epidermis, or surface, of the skin (see Anatomy of the Skin, page 2). As part of regular skin maintenance, squamous cells are constantly shed, and new cells replace the older ones. When squamous cells grow out of control, they become cancerous, developing into cSCC.
cSCC sometimes starts as actinic keratoses, a pre-cancerous skin condition caused by too much sun exposure. Commonly, it appears on sun-exposed areas of the body, such as the face, ears, neck, lips, arms and backs of hands. It can also develop in scars or chronic skin sores elsewhere. Less often, cSCC forms in the skin of the genital area. It may look like a red bump, scaly patch or sore that does not heal (see Figure 1).
cSCC is sometimes called squamous cell carcinoma of the skin or squamous cell skin cancer to differentiate it from other types of squamous cell carcinoma that are not skin cancer.
Surgery
Cryotherapy, also called cryosurgery, is a treatment that uses an instrument to freeze and destroy abnormal tissue.
Curettage and electrodesiccation is the removal of tissue with a spoon-shaped instrument that has a sharp edge. A needle-shaped electrode is then used to treat the area with an electric current that stops the bleeding and destroys remaining cancer cells around the edge of the wound. It may be repeated to ensure all the cancer has been removed. It is commonly used for small, thin cSCCs with a low risk of returning.
Shave excision is shaving off the top layers of skin, including the tumor, with a small surgical blade. It is used for small cSCCs with a low risk of returning.
Standard excision is commonly used and involves removing the tumor and a margin of normal skin around it.
Mohs micrographic surgery may be performed by a specialist when the goal is to save as much healthy skin as possible. Mohs surgery allows the surgeon to examine the margins under a microscope on the same day of surgery to confirm that all the cancer cells have been removed. It is often used when the cancer is on a place on the body that is very visible, such as the face or ears, and has a high risk of returning.
The patient is awake during this procedure. See page 2 to learn more about Mohs surgery.
Lymph node dissection may be used for some cSCCs that are very large or have grown deeply into the skin, and for lymph nodes that are hard and/or enlarged.
Radiation Therapy
Radiation therapy can be used alone or in combination with other treatments. It is sometimes used as adjuvant therapy after surgery to kill any remaining cancer cells, or if a high risk of recurrence exists. It is also used to treat areas of cSCC that are difficult to treat surgically, such as those on the eyelid, nose or ears, or for a very large tumor. It may be a preferable option for people who are not able or do not want to have surgery or who may prefer to manage the cancer instead of remove it. Radiation therapy cannot, however, be used in the same place more than once.
The schedule for each person will vary but commonly includes two to four visits a week for several weeks.
Immunotherapy
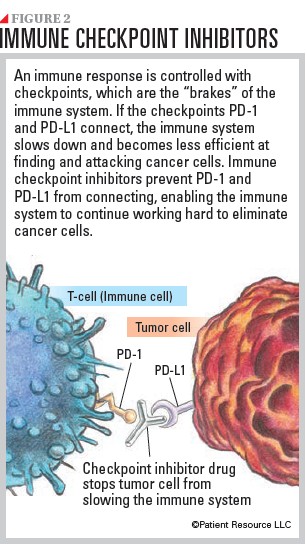
Immune checkpoint inhibitors are the form of immunotherapy used to treat advanced cSCC tumors (see Figure 2). They are a type of monoclonal antibody designed to help the immune system better recognize that cancer cells are foreign to the body. This, in turn, allows the immune cells to better destroy the cancer.
Immune checkpoint inhibitors block the receptors of PD-1 and PD-L1. PD-1 is a protein on the surface of T-cells that helps keep the body’s immune responses in check. PD-L1 is a protein found on some types of cancer cells. When PD-1 attaches to PD-L1, it stops the T-cell from killing the cancer cell. PD-1 and PD-L1 inhibitors keep PD-1 and PD-L1 proteins from attaching to each other, which allows the T-cells to kill cancer cells.
These immunotherapy drugs are typically given as an infusion into a vein, usually every two to six weeks, depending on the specific drug. The goal is to shrink or slow the growth of the tumors.
Clinical Trials
Talk with your doctor early on about the possibility of including a clinical trial in your treatment plan at some point during your care.
Some medications for cutaneous squamous cell carcinoma
- cemiplimab-rwlc (Libtayo)
- cosibelimab (Unloxcyt)
- pembrolizumab (Keytruda)
As of 7/11/25
