

Skin Cancers
Understanding Your Diagnosis
Because not every skin cancer diagnosis is the same, understanding your diagnosis begins with learning about how cutaneous squamous cell carcinoma (cSCC), basal cell carcinoma (BCC) and Merkel cell carcinoma (MCC) are diagnosed. Some of the tests and procedures may vary by skin cancer type, but many are the same. The results will be crucial for your doctor to determine the most appropriate treatment plan for you.
Biopsy Tests
Skin cancers are diagnosed based on multiple tests, but a biopsy is the most reliable way to determine which type of skin cancer you have. A biopsy is the removal of cells or tissues for examination by a pathologist, a doctor with special training to diagnose disease. Following are some types of biopsies that may be used to diagnose skin cancer:
- Excisional biopsy removes an entire lump or suspicious area as well as some healthy tissue around the abnormal area.
- Incisional biopsy removes only a sample of abnormal tissue or part of a lump or suspicious area.
- Shave biopsy removes a skin abnormality and a thin layer of surrounding skin using a small blade.
- Punch biopsy removes a small round piece of tissue, usually the size of a pencil eraser, using a sharp, hollow, circular instrument. May require a stitch or suture.
- Sentinel lymph node (SLN) biopsy surgically removes the sentinel node(s), which is the first lymph node to which cancer is likely to spread from the primary tumor.
- Needle biopsy removes tissue or fluid with a needle.
- Core biopsy uses a wide needle to remove tissue or fluid.
The information obtained from your biopsy will be noted in a pathology report, which is the description of cells and tissues made by a pathologist based on microscopic evidence. It will be used to diagnose and stage your skin cancer, and it will guide your doctor in selecting treatment options. You may request a copy of your pathology report at any time.
Sentinel Lymph Node (SLN) Mapping
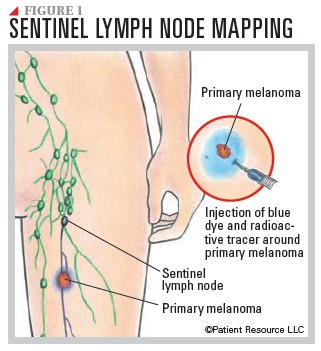
If your doctor suspects the skin cancer has spread to nearby lymph nodes, sentinel lymph node mapping may be recommended. Accurately identifying which lymph node is the SLN is important for many reasons. The decision to remove lymph nodes often depends on whether there is concern that the cancer has spread to an SLN. SLN mapping tracks the exact path of the bodily fluid (lymph) that carries white blood cells as it drains from the skin surrounding the primary tumor to the nearest lymph node. The draining lymph node closest to the primary tumor is called the sentinel lymph node.
SLN mapping uses lymphoscintigraphy, a special type of imaging technique done in a hospital’s nuclear medicine department. Ideally, it is performed on the same day as surgery to remove the primary tumor. A radioactive tracer is injected into the skin around the site of the primary tumor, and an imaging device that detects radioactivity makes a series of images that show the path of the radioactive material as it travels to the nearest group of lymph nodes. The surgeon injects a special dye into the skin around the site of the skin cancer to visually identify the SLN. The surgeon then makes a small incision in the area of the lymph nodes and removes the SLN. The node(s) are carefully examined by a pathologist for the presence of cancer cells. Because the SLN is the first place to which lymph drains from the site of the skin cancer, it is unlikely the cancer will have spread to other lymph nodes if no cancer cells are found in the SLN (see Figure 1).
An SLN biopsy is not commonly used for BCCs because they tend not to spread. In cases where BCC is considered high-risk and has spread to lymphatic vessels within the primary tumor, an SLN biopsy may be performed.
An SLN biopsy may be performed on some cSCCs if the cancer is high-risk, if it is suspected that the cancer has spread to the lymphatic vessels, if lymph nodes near the tumor are enlarged or if the cancer has metastasized.
Additional Tests
Further testing may be required for diagnosis.
Imaging tests may be performed to determine the depth of the cancer, whether the skin cancer has spread, how well treatment is working or to look for possible signs of a recurrence after treatment. These tests include computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (PET), PET/CT and PET/MRI.
Blood tests may be included in the diagnostic tests. These may include blood cell counts and blood chemistry levels as well as checking your kidney and liver function before treatment begins. In cases where MCC is suspected, your blood may be tested for antibodies to the Merkel cell polyomavirus (MCV), which has been found to cause a majority of MCC diagnoses. Blood tests may also be used to check for antibodies to the virus to monitor whether treatment is working. If treatment is working, MCV antibodies should decrease. If they increase, it is possible the cancer has returned.
Immunohistochemistry is a test performed in a laboratory on a biopsy sample. This test is used primarily for MCC because the “small round blue cell” histologic pattern of MCC must be differentiated from several other tumors, such as small cell lung carcinoma, carcinoid tumor, malignant lymphoma and small cell melanoma. Immunohistochemistry uses antibodies to check for certain antigens (markers) in a sample of tissue. The antibodies are usually linked to an enzyme or fluorescent dye. After the antibodies bind to the antigen in the tissue sample, the enzyme or dye is activated, and the antigen can then be seen under a microscope.
Genetic testing may be done for people with BCC or cSCC who have certain genetic syndromes that increase their risk of getting this type of skin cancer. These syndromes include the following:
- Gorlin syndrome, also known as basal cell nevus syndrome, is a rare inherited genetic mutation in one of the tumor suppressor genes that causes the development of multiple basal cell skin cancers, jaw cysts and skeletal abnormalities.
- Xeroderma pigmentosum is where the body is not able to repair damage to DNA from sunlight. Skin with a lot of DNA damage can become skin cancer.
- Muir-Torre syndrome involves a mutation in DNA mismatch repair genes leading to multiple cSCCs and other cancers.
- Recessive dystrophic epidermolysis bullosa, a rare, inherited skin disorder, causes the skin to become very fragile and causes painful blisters.
Meet the Team
You will likely meet more than one type of health care provider during the course of treating your skin cancer. Following are some of the health care professionals that may be on your team.
Dermatologists are trained to diagnose and treat skin problems.
Pathologists are trained to identify diseases by studying cells and tissues under a microscope.
Dermatopathologists have special training in looking at skin samples.
Mohs surgeons perform a specialized surgery called Mohs micrographic surgery, which removes a thin layer of tissue around a skin cancer. Each layer is examined under a microscope. If cancer cells are seen, thin layers of tissue are removed until no cancer cells are seen.
Head and neck surgeons are specially trained to perform surgery, such as sentinel lymph node (SLN) biopsy, on the head and neck area.
Medical oncologists treat cancer with drug therapy or other medications.
Oncology nurses provide inpatient or outpatient care in a cancer treatment facility.
Pharmacists prepare and dispense prescription drugs. They are also a resource for drug-related information.
Plastic surgeons are trained to reduce scarring or disfigurement by surgically reconstructing facial and body tissue.
Radiation oncologists are trained to use radiation therapy to treat cancer.
Surgical oncologists perform biopsies and other surgical procedures.
Genetic counselors are specially trained in medical genetics and counseling. They help people find out if they have a genetic condition and help them understand their genetic test results.
Myths vs Facts
Myths about skin cancer prevent people from properly protecting their skin. Following are some common myths about skin cancer and the facts behind them.
Myth: Skin cancer only affects fair-skinned individuals.
Fact: Skin cancer can develop in people of all skin tones, including those with darker skin.
Myth: A tanning bed is safer than UV rays from the sun.
Fact: The ultraviolet light from tanning devices can be harmful because UV radiation can damage your skin. Avoiding all tanning devices is recommended.
Myth: You don’t need to wear sunscreen on a cloudy day or during the winter.
Fact: It is possible for the sun to harm your skin and eyes even on cloudy days. Harmful rays are present year round.
Myth: Skin cancer only affects older adults.
Fact: Although damage done to your skin in your youth may not become cancerous for many years, anyone can get skin cancer at any age.
Myth: A base tan prevents sunburns.
Fact: There is no such thing as a “safe” or “base” tan that prevents sunburns. Ultraviolet rays, whether from the sun or a tanning device, damage the DNA of your skin cells.
Myth: Skin cancer only occurs on sun-exposed areas of the body.
Fact: Skin cancer can develop anywhere on the body, including areas not typically exposed to the sun, like the soles of the feet, palms, under fingernails and genitals.
Myth: If your routine doesn’t include any outdoor activities, you are not at risk of getting skin cancer.
Fact: Dermatologists say brief sun exposures throughout the year can add up to significant damage for people with fair skin. These cumulative, everyday exposures are linked to cSCC. Exposure to certain chemicals, like arsenic, coal tar and some petroleum products, can increase the risk of skin cancer. Some occupational exposures, such as those in the oil industry, can also lead to increased risk.
Myth: Suspicious moles can just be cut off by the doctor before they become cancerous.
Fact: Don’t rely on that as a quick fix. If you see a sore that won’t go away or a mole that has changed size or color, it could be an early form of skin cancer and needs to be checked out.
